While presenting earlier on this year at the British Fascia Sympoium, I was fortunate enough to meet Dr. Wilbour Kelsick. A veteran member of the official staff for the Canadian National and Olympic teams.
Dr. Kelsick believes that optimal health is the result of balance in several areas of life. Wilbur looked at fascial training principles in running. We looked at the fluidity required in a running posture, plus the importance of minimal muscular tension but enough tension to hold the body together as a bio-tensegrity structure. When we walk and run we need effective application of force and need to feel as if we are walking through something. As we speed up we should feel as if we are stepping over something. Our foot arches acts as springs as they store elastic energies. We need to spend more time off the ground rather than on the ground. Try listening to the landing of the runner, the footprint is a dead giveaway to what is going on in the gait pattern.
 So how can movement therapist get involved and help runners along their journey?
So how can movement therapist get involved and help runners along their journey?
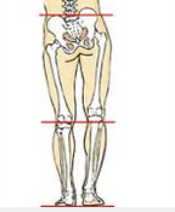
The runner is always at risk for development of injury to the hip and pelvis secondary to chronic repetitive micro trauma. Evidence for preventive strategies to lessen running injuries is needed as these occur in 40%-50% of runners on an annual basis. Many factors influence running injuries from posture, footwear and floor surface, but strong evidence for prevention only exists for training modification primarily by reducing weekly mileage. Two anatomical factors – cavus feet (high arch on middle of the foot) and leg length inequality (usually coming from pelvis) – demonstrate a link to injury and trauma.
When runners attend my sessions one of things I start off with is establishing the lumbo pelvic rhythm and getting the client to use the GYROTONIC pulley tower. We establish ground force reaction through the feet (grounding), the spiral line through the pressure of the big toe, the natural arch and curl in the spine and the hip flexion, extension on the seated pelvis, feeling the head of the femur going towards and away for the ASIS and rotation and twist through the upper extremity.


The key to treatment is establishing complete and accurate diagnosis, and, in particular, identifying the functional bio-mechanical deficits in the kinetic chain that contribute to this repetitive micro trauma.2
A long-term successful outcome and prevention of re-injury are more likely if the focus of rehabilitation is on the restoration of the functional kinetic chain, rather than on a specific injured tissue. For example, the typical treatment of “iliotibial band syndrome” is a stretching protocol that frequently is unsuccessful in the long-term improvement of symptoms.3
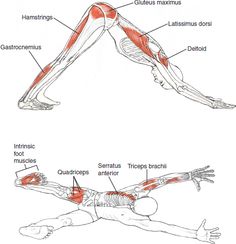
From my dissection experience the iliotibial band only exists because we cut it out and into that shape. A functional bio-mechanical approach may identify that the injured runner has a lack of calcaneal eversion and a structurally rigid supinated foot. Try taking your clients into downward dog and then playing with the feet by rolling them from one side to another, lifting the toes and arches and swinging the hips . Read more about the feet here:
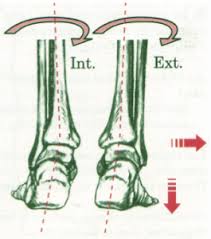
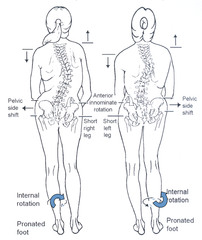
If a runner suffers from these functional biomechanical deficits they would lead to inadequate internal rotation of the tibia and femur and result in inhibition or decreased recruitment of the gluteal muscles, in particular the gluteus medius. I know this from my own personal struggles. Restoring pronation throughout the lower extremity would require joint play techniques or functional joint mobilizations for the foot and ankle. Pronation or eversion is the inward roll of the foot (medial malleolus) while walking or running. As another way to look at pronation instead in terms of the degree of inward roll is in terms of where the foot pushes off at the end of each step, or at the end of the gait cycle.
Anatomically, all asymmetric whole body activities, even those that principally involve flexion and extension, contain elements’ of twisting. 4
Take the walk or gait pattern as we step forward the opposite arm comes forward creating moderate twist, this not only balances the bodies but calms the central nervous system. We should also introduce torque in the body. What is Torque? Torque is a mechanical force that produces a rotation. It is imitated by connective tissues effort and does not have to produce a visible result. It can accentuate a twist or have an an static (isometric effect) like trying to open a door knob and failing, it just wont turn.
The movement practitioner thinks of rotation in the spine, there are in fact 24 such rotations in between c1 and the sacrum – this adds up to a lot of movement, even though this takes place against the resistance of intervertebral discs, facet joints between vertebral arches, the rib cage, and muscles and ligaments from head to pelvis. We rarely do complete spinal twist in every day life but they are fundamental in Hatha yoga, Pilates and GYROTONIC. This is so important to a runner and also during the pre-hab and rehabilitation phase of training.
Swivels are another sort of twisting often seen to the extreme in sports like skiing. For example when a skier goes through a steep drop with short side to side excursions while keeping the shoulders perpendicular to the fall line of the downhill slope. In everyday life we face the torso in a different direction other than straight ahead but then swivel at the hips. Any sort of twist in Yoga, Pilates and GYROTONIC will involve medial rotation of one thigh and lateral rotation of the other.

If you want to think of muscles working in isolation a way to do so on the twist is when we twist to the right, it’s the right external and left internal oblique that shorten concentrically and the right internal and left external oblique that lighten against resistance.
Compression- trying to twist when we are working in compression is a no. By this I mean restoring the body to as near as it can to neutral, but having the ability to coil and recoil in and out of neutral. Oblique muscles create twists and horizontal muscles resist them isometrically. Every time we do a spinal twist the obliquely and vertically muscles compress the spine.
In conclusion if we have good elasticity in our fascial systems we will spend minmum time on the ground when running.
Bibliography
Anatomy of Hatha Yoga- David Coulter
Evidence-based treatment of hip and pelvic injuries in runners- http://www.ncbi.nlm.nih.gov/pubmed/16005401 – 2, 3, 4
Prevention of running injuries – http://www.ncbi.nlm.nih.gov/pubmed/2046350