So I speak from experience here as i’ve had over 30 years in the fitness and dance business; 25 of those years were as a pilates/yoga teacher, and just under 20 years of those were owning commercial studios. Here are five of the many anatomy myths that i’ve encountered over the years. I now offer consultancy to studios and teachers and also anatomy modules for manual and movement therapist. I am constantly approached by market research companies plus advanced physio students running market research campaigns on the some of the points below.
As therapists or medical practitioners, we should always be questioning our belief system every day.
The five points I discuss below I have experienced with studios, class participants, workshops, books and training across the world. Again it is not that the teacher or therapist is wrong or right, it’s the way they have been taught in their system. I have seen this in physiotherapy, chiropractors, sports massage, osteopathy, Feldenkrais, cranial sacral therapy, naturopathy and surgical operations. There are many other ways of looking at the body. If we stay in one mindset we only become the best possible us based on our own limited beliefs.
- Pilates and Yoga will be the miracle medicine and cure that bad hip, that knee, that cancer, that arthritis, that depression and the list goes on. By doing asana X, Y and Z or by doing Pilates exercise A, B and C you will cure yourself of that ailment or symptom. So this is a very standard statement and one size does not fit all. We are all different, so what works for one person may not work for another. Pilates and Yoga have many benefits and outstanding results. This can clearly be seen across communities around the world, helping with everything from cancer to that frozen shoulder. This has been documented medically on a number of research papers. If we are teaching generic group classes, many of us will say this exercise or movement will do such a thing. However for some people this may be the opposite, it may make their condition worse and give them false expectations. It’s really important to “assess rather than guess.” We should educate the class participant by guiding them rather than trying to fix them. After all, fixing a client makes the client reliant on the the therapist rather than empowering them with the information to think and take charge for themselves. Without considering other aspects of the clients life such a physiological load, we could be leading the client up the wrong path. ‘Motion is definitely lotion’ and ‘there is no such thing as a bad exercise, but there is such thing as a badly prescribed exercise’. However we do have to look at the bigger picture.
 Case study 1 – Joe Bloggs is a plumber, he calls me and tells me he has spent £1000’s of pounds on all sorts of orthopaedic consultants to manual and movement therapists and nothing has worked to reduce his back pain and improve his flexibility. It’s not that any of those treatments were wrong, just they are not working in conjunction with one another. He desperately needs to improve his flexibility and has been told that yoga will improve his present condition. He wants a guarantee in writing from me stating that if he spends X amounts of pounds and so many hours doing yoga he will achieve his expectations. He has tried numerous yoga classes with no avail. I book him in for a one to one consultation. On arrival he is agitated, cross, frustrated and needs help and guidance. I find he is sympathetic dominant and his diet is rich in carbohydrates and sugar and will thus keep him sympathetic dominant and mouth breathing. When I start to move him, he is so full of tension and rigidity that his body cannot relax into any sort of state that would be inducive to better breathing, parasympathetic dominant to induce flexibility. I invite him to be a client of mine but tell him reducing his back pain and increasing his flexibility will depend on what goes on outside the studio in the other weekly hours rather than in. It’s not what he wants to hear, and leaves disappointed. I of course wish him well and really hope another therapist or surgeon can help him using a different approach.
Case study 1 – Joe Bloggs is a plumber, he calls me and tells me he has spent £1000’s of pounds on all sorts of orthopaedic consultants to manual and movement therapists and nothing has worked to reduce his back pain and improve his flexibility. It’s not that any of those treatments were wrong, just they are not working in conjunction with one another. He desperately needs to improve his flexibility and has been told that yoga will improve his present condition. He wants a guarantee in writing from me stating that if he spends X amounts of pounds and so many hours doing yoga he will achieve his expectations. He has tried numerous yoga classes with no avail. I book him in for a one to one consultation. On arrival he is agitated, cross, frustrated and needs help and guidance. I find he is sympathetic dominant and his diet is rich in carbohydrates and sugar and will thus keep him sympathetic dominant and mouth breathing. When I start to move him, he is so full of tension and rigidity that his body cannot relax into any sort of state that would be inducive to better breathing, parasympathetic dominant to induce flexibility. I invite him to be a client of mine but tell him reducing his back pain and increasing his flexibility will depend on what goes on outside the studio in the other weekly hours rather than in. It’s not what he wants to hear, and leaves disappointed. I of course wish him well and really hope another therapist or surgeon can help him using a different approach.
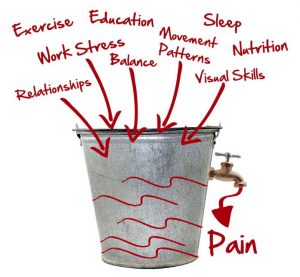
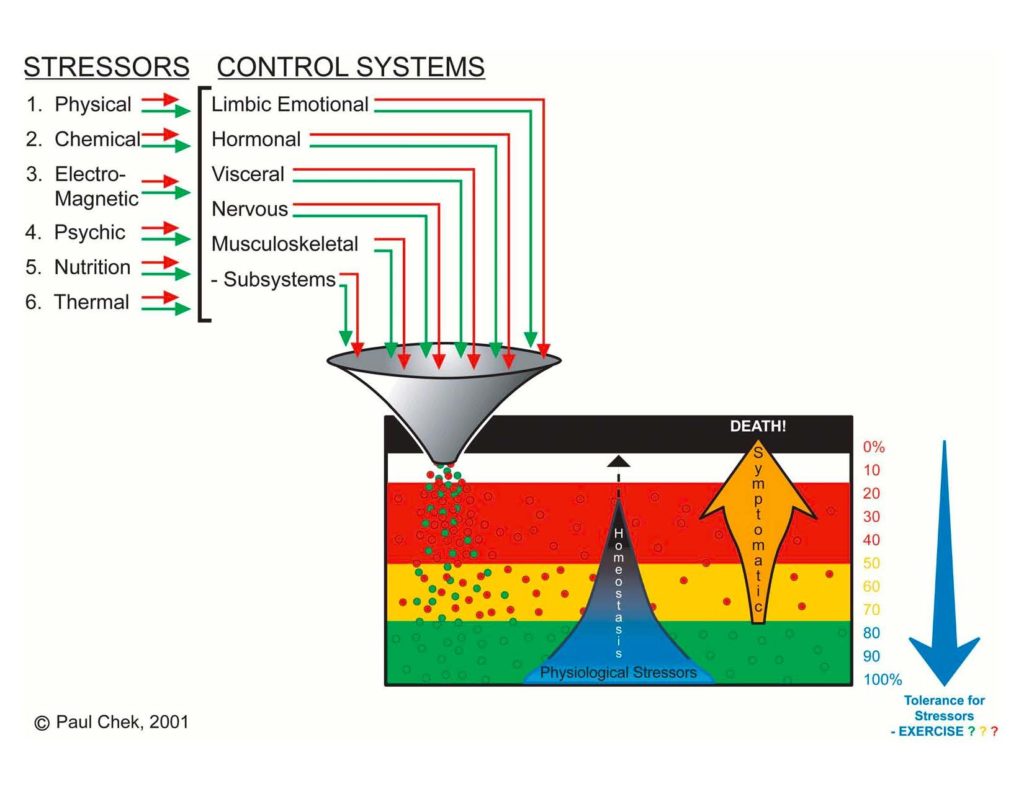
The image below is one of Paul Chek’s showing the different variables that influence the body. I always give any pain or chronic injury client the choice as a responsible adult, to whether they want to treat the symptom or the root cause.
2. If you keep stretching and putting in the hours you will be able to do the splits, the back bend, the forward fold and the list goes on. So there are so many variables out there that effect a persons flexibility. Most schools of movement teach that mobility is dependent on the connective tissue, i.e muscle, ligaments, tendons and fascia. However they are missing two really important points. The first being the joint shape, angle of joint, genes and environment. Paul Grilley master of yin yoga detailed how joint shape , particularly pelvic shape, femur length, and shaft head position would greatly influence movement and yin postures. Stuart McGill seconded this by talking about dalmation hip and ethnic origin. Read more on hip shape here.
‘Beighton scale’ provides a great starting point for flexibility. I know after running a dance school for over 16 years that some children genetically have flat turn out and will be accepted at the Royal ballet school, whereas other children would strain and cause injury to surrounding tissues trying to get what is not really achievable. The second point everyone is missing is the central nervous system. It has been shown in cadavers that living clients with restrictions in the body are suddenly able to move the full shoulder joint when deceased. Thus, this tells us that the central nervous system was key in their range of motion (and this is an article in itself – panjabi system).
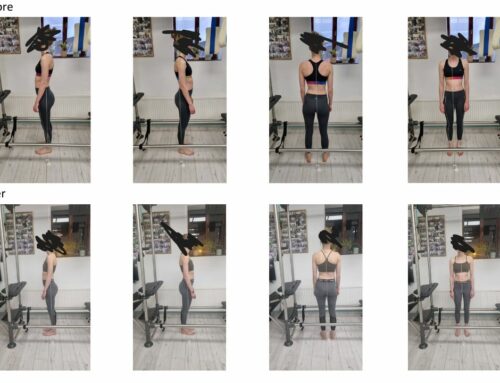
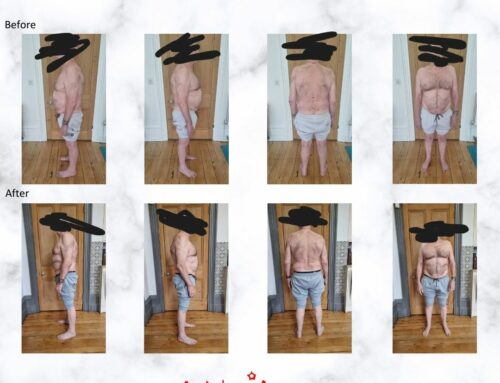
3. The anatomy book states that when we do a particular exercise or asana, only specific muscles are firing, as in the pictures below. These images are brilliant, allowing one to focus on particular muscles. Just like physiotherapy, getting a client to focus their intention and attention to particular area or muscle group can greatly influence the effect of movement or asana. However, what is then forgotten is the rest of the body, including fascia and bones.
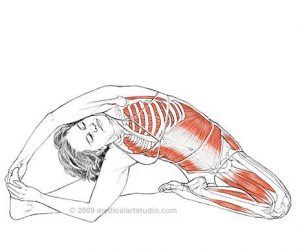
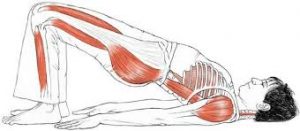
 Also, everyone is different, meaning certain areas may be over facilitated – short and tight or long and taut – or under active and weak. All muscles are a combination of both slow and fast twitch fibres. Our body is a reflection of our life and emotions, body and mind cannot be separated. Put simply, are the postures below going to look the same as the asanas above?
Also, everyone is different, meaning certain areas may be over facilitated – short and tight or long and taut – or under active and weak. All muscles are a combination of both slow and fast twitch fibres. Our body is a reflection of our life and emotions, body and mind cannot be separated. Put simply, are the postures below going to look the same as the asanas above?
 4. Hold your stomach in, it’s the best thing for you to stabilise plus you never know who is watching. Through this, you will get rid of all pain and have a flat tummy and perfect posture. The stomach should naturally go in and out with the breath, technically two thirds of the breath should start in the belly and expand; the final third will go up into the lungs (rib expansion, diaphragmatic breathing). When we restrict the breath by permanently holding the stomach in we can cause a reverse breathing pattern and over facilitation of the upper trunk and neck muscles. This shows up as other problems such as TMJ (and the list goes on). The tranversus abdominus should naturally engage prior to any movement. We can cue in the engagement of the core on certain exercises such as the dead lift, because of the load. Also core engagement can be cued when doing certain pilates exercises such as the series of five and yoga bandhas.
4. Hold your stomach in, it’s the best thing for you to stabilise plus you never know who is watching. Through this, you will get rid of all pain and have a flat tummy and perfect posture. The stomach should naturally go in and out with the breath, technically two thirds of the breath should start in the belly and expand; the final third will go up into the lungs (rib expansion, diaphragmatic breathing). When we restrict the breath by permanently holding the stomach in we can cause a reverse breathing pattern and over facilitation of the upper trunk and neck muscles. This shows up as other problems such as TMJ (and the list goes on). The tranversus abdominus should naturally engage prior to any movement. We can cue in the engagement of the core on certain exercises such as the dead lift, because of the load. Also core engagement can be cued when doing certain pilates exercises such as the series of five and yoga bandhas.
With regards to lower back , yes cores support will help, but the pain doesn’t just happening isolation, it is usually a combination of issues that can cause the flare-up. Focusing on the connection of the front muscles into the insertion of the main junction box (the thoracolumbar fascia), we can help to avoid strain and pain on the lower back. Engaging the core is correct when understood and taught properly and does provide trunk stabilisation (Hodges & Richardson). This does not mean holding the breath for long periods of time. What most therapists and medical professionals are missing is that optimal trunk stabilisation cannot happen optimally if there is chronic inflammation in the gut, intestinal wall, small and large intestine or colon. Inflammatory foods coming into the system will affect intrinsic core stabilisation. Reducing foods that inflame the small intestine will help the muscles situated at the front of the pelvis to work more efficiently, helping stabilise the lumbopelvic region.

A 1997 medical research paper stated:“Activity of the trunk muscles is essential for maintaining stability of the lumbar spine because of the unstable structure of that portion of the spine. Trunk muscle activity occurring prior to activity of the prime mover of the limb was associated with hip movement in each direction”. ( Hodges and Richardson,Physical Therapy, Volume 77, Issue 2, 1 February 1997, Pages 132–142,)
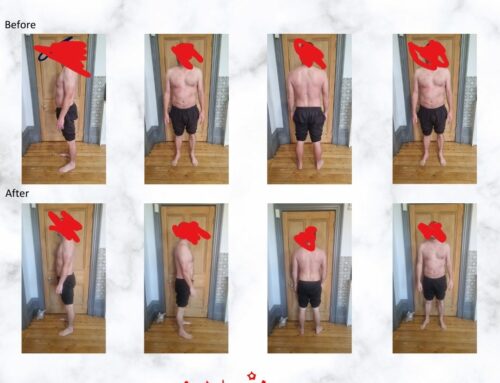
5. “Your feet should be together not apart; your body should be in this position; start here, finish here like the original asana or the original Joseph Pilates exercise.” It’s not about teaching a series of movements or set asanas to people. It’s about adapting the asanas and movement practice to the client in front of you. We should also look at where they are emotionally, physically, mentally and spiritually. Also, what is their body type and are they going to achieve that position with ease? Is it going to strain and cause them further tension? Do they get the quality and essence of what they should or should not be doing? Is there a wrong or right way to be doing this?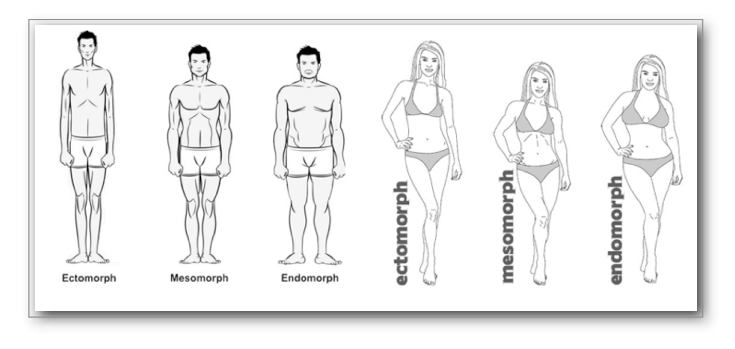
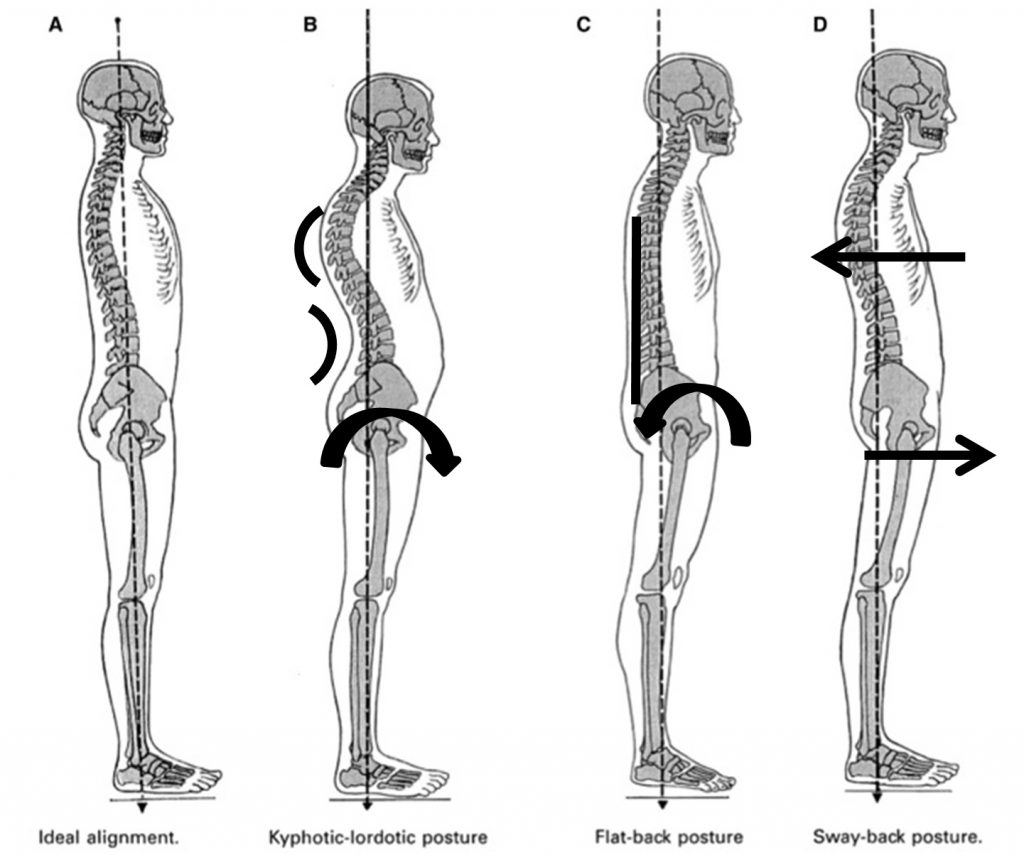
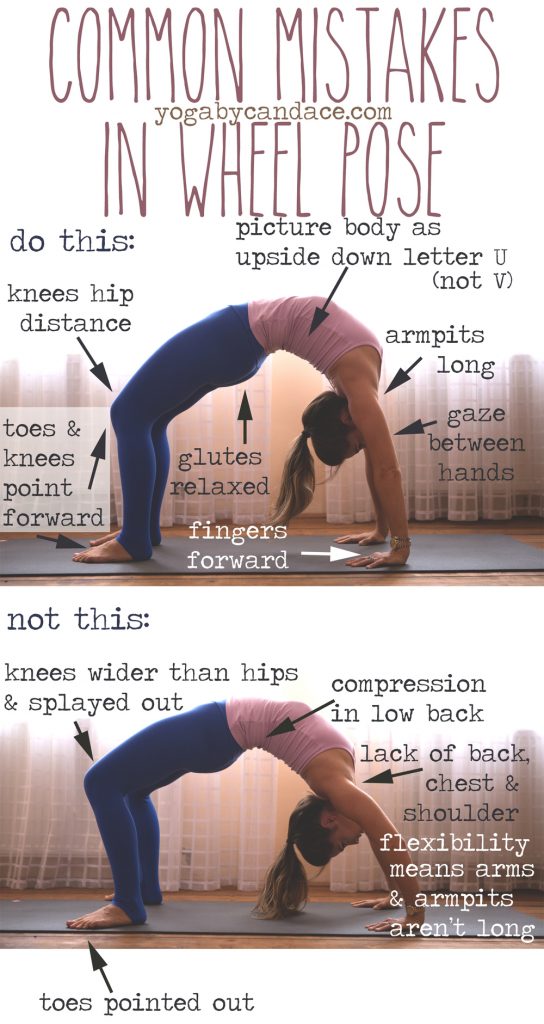 The picture of the wheel (to the right) is both used on the pilates reformer and in yoga asana. The picture shows clearly what they call wrong or right. My analogy is different, the picture shows where the client does not have range of movement in the hips (creating space by rotating the feet out). In the thoracic spine, the last 40 degrees of shoulder flexion requires thoracic extension. Clearly, this person does not have the range of motion required to do the perfect asana – full stop. Therefore the lumbar spine becomes compressed . They also don’t have optimal hip extension. The reason for this will all be a cocktail of many causes; just because the picture is not perfect does not mean the person is wrong. Instead, they are working to the best of their ability, and this is were they presently are.
The picture of the wheel (to the right) is both used on the pilates reformer and in yoga asana. The picture shows clearly what they call wrong or right. My analogy is different, the picture shows where the client does not have range of movement in the hips (creating space by rotating the feet out). In the thoracic spine, the last 40 degrees of shoulder flexion requires thoracic extension. Clearly, this person does not have the range of motion required to do the perfect asana – full stop. Therefore the lumbar spine becomes compressed . They also don’t have optimal hip extension. The reason for this will all be a cocktail of many causes; just because the picture is not perfect does not mean the person is wrong. Instead, they are working to the best of their ability, and this is were they presently are.
Bibliography
Paul Chek blogs
Billy Whittle facebook